
Anatomy of the Tibial Eminence
The knee joint is made up of bones, the thighbone, and shinbone (lower leg), which articulate with each other. The upper aspect of the shinbone is made up of the medial (towards the inner side of the knee) and lateral (towards the outer side of the knee) plateaus (flat regions). Between these plateaus, the bone is raised to form the tibial eminence. The tibial eminence consists of the medial and lateral spines. The medial spine provides attachment for the anterior cruciate ligament (ACL).
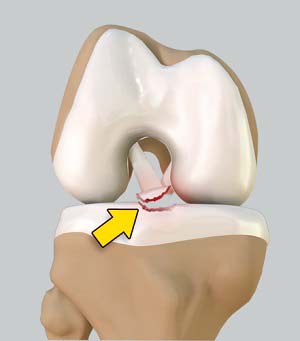
What is Tibial Eminence Spine Avulsion Fracture?
Tibial eminence spine avulsion fracture is the avulsion (tearing away) of the tibial eminence.
Causes for Tibial Eminence Spine Avulsions
This injury may occur because of abnormal outward bending or twisting injuries caused by a sudden halt of moving joints, excessive flexion (bending inwards) and internal rotation, which usually occur during skiing and motor vehicle accidents.
Types of Tibial Eminence Spine Avulsions
Tibial spine avulsions are classified into:
- Type I: Non-displaced or minimally displaced spine avulsion
- Type II: Fracture is rotated but the rear end or posterior part of the avulsion is still in place
- Type III: Completely displaced fracture
Treatments for Tibial Eminence Spine Avulsions
The treatment options for tibial spine avulsions include
- Extension casting for type I fracture
- Extension casting or open reduction and internal fixation (ORIF) if required for type II fractures
- ORIF for type III injuries
The injured knee is placed on a leg holder over the radiolucent operating table as postoperative plain X-rays will be taken after the procedure to verify whether reduction and fixation are satisfactory.
In a minimally invasive arthroscopic procedure, tiny incisions are made on the front of the joint. The arthroscope is inserted through an anterolateral portal (from the side) while the probe and other instruments are passed through an anteromedial portal (from the center). The hematoma (localized bleeding) is removed at first using motorized suction shaver. The fragments are identified and all soft tissues around them are debrided for proper viewing of the joint. The knee is examined for any entrapped meniscus or intermeniscal ligament and any interposing soft tissue is pulled back so that the avulsion fracture can be reduced with an arthroscopic probe applying firm and gentle pressure.
The bone can be fixed in place using either screws or non-absorbable sutures. Screw fixation is a very good technique when the bony fragment is large enough and in adults when the growth plate is closed or fused completely. A non-absorbable suture fixation technique may be considered in children in whom the growth plates are not fused and in conditions in which the fragment is not sufficiently large enough to accommodate a screw.